
Why Your Ribs Keep "Going Out" — And What to Actually Do About It: Costovertebral and Costotransverse Joint Dysfunction in Hypermobility
If you've ever felt a sharp or burning pain in your upper back — between your shoulder blade and your spine — that gets worse when you breathe deeply, reach overhead, or twist, and sometimes comes with a popping or clicking sensation, there's a good chance you've experienced costovertebral or costotransverse joint dysfunction. And there's an equally good chance no one has ever told you that's what it is.
This is one of the most common conditions I see in people with connective tissue hypermobility, and one of the most consistently undiagnosed. Not because it's rare or hard to understand — but because it requires hands-on assessment of specific joints that most providers simply aren't examining.
The anatomy: what these joints are and why they matter
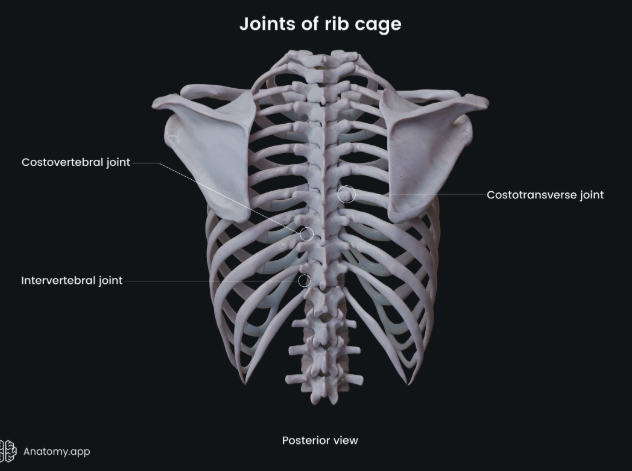
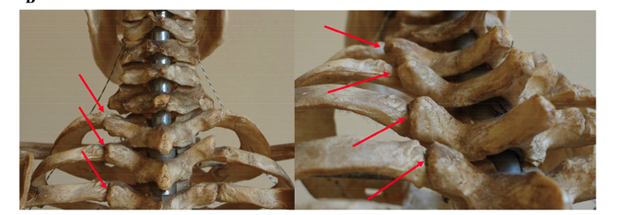
Your ribs each connect to your thoracic spine through two small gliding joints: the costovertebral joint (where the rib head meets the vertebral body) and the costotransverse joint (where the rib tubercle meets the transverse process of the vertebra). This two-point connection exists at ribs 1 through 10. The 11th and 12th ribs — the floating ribs — have no costotransverse joint, and no intra-articular ligament, which is part of why those ribs behave differently.
These two joints don't work in isolation. They function as a coupled mechanical unit — specifically, a first-class lever system, where the costotransverse joint acts as the fulcrum and the rib head and posterior vertebral body are the two opposing levers [1]. You can't move one without affecting the other, which is why dysfunction here tends to involve both joints together.
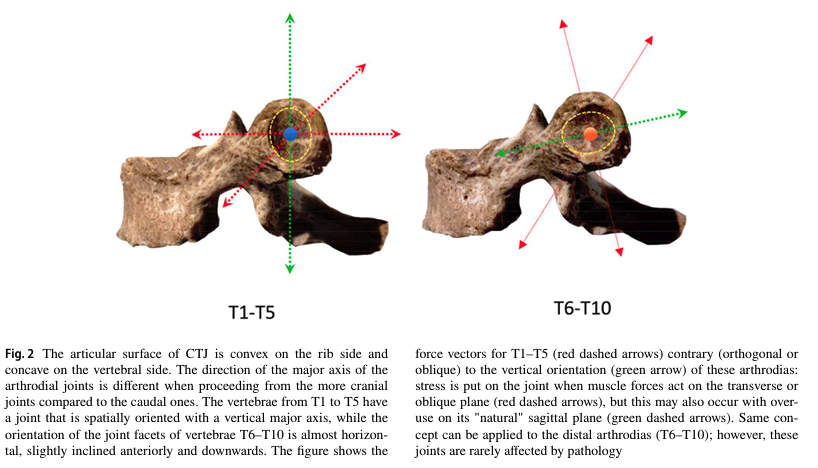
The orientation of the joint facets changes as you move down the spine, and this matters clinically. The upper five costotransverse joints (T1-T5) have a near-vertical major axis, so those ribs are designed to move primarily in the sagittal plane — forward and back with breathing. The lower joints (T6-T10) are oriented nearly horizontally, and their movement occurs on the transverse plane [1]. When forces act on either joint in a direction other than its usual plane of movement, stress accumulates in the joint capsule and surrounding ligaments. Over time — or acutely, in a hypermobile individual — that stress produces inflammation, pain, and sometimes subluxation.
These joints are also richly innervated. Research has confirmed the presence of substance P and calcitonin gene-related peptide (CGRP) within the costovertebral joint capsule and synovial tissue — the same neuropeptides involved in pain sensitization and neurogenic inflammation [2]. The thoracic sympathetic trunk provides additional innervation to the joint capsule [3], which means these joints are capable of producing both somatic and autonomic pain responses. That's part of why the pain from this area can feel so diffuse, burning, and difficult to pin down.
Why you're probably undiagnosed
In a 1992 case series published in the Postgraduate Medical Journal, five patients with atypical chest pain arising from costovertebral dysfunction had each undergone extensive cardiac and pulmonary investigation — including multiple EKGs, chest X-rays, and pulmonary workups — before the correct diagnosis was finally made [4]. This pattern is still common today.
Here's why:
Standard imaging misses it. X-rays and MRIs of the thoracic spine typically look normal. Musculoskeletal ultrasound is actually the recommended first-line imaging approach: research has shown it can identify joint effusion (fluid collection in the joint capsule) that correlates 100% with the patient's reported site of pain [1]. The problem is that most providers don't know to look there, and when they do order imaging, ultrasound of these joints isn't on most standard protocols.
The symptoms mimic other things. Costovertebral and costotransverse pain can radiate anteriorly around the rib cage, producing chest tightness or pressure that looks like a cardiac or pulmonary problem. Irritation of the posterior branches of the thoracic spinal nerves at these joints can produce a burning quality that gets attributed to neuropathy or anxiety [1]. And in a population that's already been told their pain is "just anxiety" or "just hypermobility," adding another misdiagnosis to the pile is unfortunately easy.
Most providers aren't examining for it. Identifying dysfunction at these joints requires hands-on palpation of the rib head and assessment of its movement relative to the spine — something not included in a standard physical exam. Even within physical therapy, specific rib and costotransverse assessment requires training beyond the typical curriculum.
A note specific to the hypermobility population: the existing published literature on costotransverse joint pathology has been developed primarily in people without connective tissue disorders. The hypermobility piece — ligamentous laxity, instability, recurrent subluxation — represents a genuine gap in the current evidence base. What we know about these joints is being applied to a population whose presentation is meaningfully more complex, and the literature itself acknowledges that "the pathophysiology of this disorder is not yet completely clear" [1].
Why it happens: causes in the hypermobile population
Movement patterns and overuse(research-supported)
Because the costotransverse joint serves as the mechanical fulcrum for rib movement, it's subject to significant force in everyday activity. Published research identifies the following as movements that generate off-plane stress on the upper costotransverse joints: repeated shoulder flexion, external rotation, and abduction; scapular abduction and adduction; neck flexion-extension and rotation; thoracic torsion; and rapid or heavy breathing [1]. Any of these, sustained or repeated over time, can accumulate stress on the joint capsule — particularly at the upper joints (T1-T5), which are most exposed to these force vectors.
This helps explain why the condition is more common on the non-dominant side (80% of cases in one study [1]) — a joint that moves less tends to respond more acutely when force is applied. It's also more common in women, and more common in younger individuals, for reasons that include both anatomical and hormonal factors.
Connective tissue hypermobility(research-supported )
In people with EDS, HSD, or hypermobile connective tissue disorders, the ligaments supporting the costovertebral and costotransverse joints are more compliant than typical. No published study has examined these specific joints in an EDS population directly — that gap in the literature is real. However, research on rib instability in hypermobility disorders consistently documents that excessive movement and subluxation at the rib-spine junctions occur in this population [5], and the structural mechanism is straightforward: less passive ligamentous restraint means greater reliance on active muscular stabilization, and when that stabilization fails or is temporarily overwhelmed, the joint moves further than it should.
Hormonal fluctuations(clinical application from published research)
Sex hormones directly affect ligament compliance, and this is worth taking seriously. A 2025 systematic review of 54 studies found that hormonal shifts associated with the menstrual cycle, oral contraceptive use, pregnancy, and menopause can alter ligament mechanical properties — effects mediated at least in part by relaxin [6]. Measured increases in joint laxity corresponding to peak estrogen and progesterone levels have been documented across the menstrual cycle [7]. Progesterone also upregulates relaxin receptor expression in connective tissue, amplifying the ligamentous response to relaxin during the luteal phase — a double hit.
This research comes from studies of peripheral ligaments, primarily the ACL. There are no published studies on hormonal effects specifically on costovertebral or costotransverse ligaments. The application to rib stability is a reasonable, mechanistically grounded extrapolation — not a proven fact. That said, the clinical pattern is unmistakable: many patients with hypermobility notice their ribs are harder to manage in the luteal phase, during perimenopause, in pregnancy, and postpartum. This is not in their heads, and it's not a coincidence.
Breathing pattern changes(clinical observation)
Many people with hypermobility develop compensatory breathing habits over time — upper chest breathing, shoulder elevation on inhalation, breath holding. These patterns place repeated and abnormal mechanical load on the upper thoracic rib joints with every breath cycle.
Stabilizer fatigue(clinical observation)
The rib cage requires continuous active stabilization — from the deep spinal muscles, intercostals, serratus, and diaphragm — to hold its position during movement. When those muscles are fatigued, the passive restraint system carries more load. In hypermobile individuals, that passive system is already running at a deficit.
What it feels like

Published clinical descriptions characterize the typical presentation as stabbing or burning pain in the paravertebral region, between the medial border of the scapula and the thoracic spinous processes [1, 4]. In one ultrasound study, correlation between joint effusion location and patient-reported pain site was 100%, and the upper four thoracic joints (T1-T4) were involved in 73% of cases [1].
Common features include:
Sharp or aching pain near the thoracic spine, usually close to — but slightly lateral to — the midline
Pain worsening with deep breathing, reaching overhead, twisting, or rolling over
A clicking, popping, or snapping sensation in the back or rib cage
The strong subjective sense that something is "out" or "caught"
Pain radiating around the rib cage — can feel like chest tightness or pressure
A burning quality to the pain, often attributed elsewhere
Pain with coughing or sneezing
Difficulty sleeping on the affected side
In people with connective tissue hypermobility, the presentation often includes additional features not well described in the published literature: (clinical observation)
Recurrent subluxation with minimal provocation
The rib shifting back out shortly after manual correction — sometimes with the next breath or change in position
Episodes that worsen noticeably during specific hormonal phases
Severity that feels disproportionate to observers unfamiliar with the mechanics involved
A note on rib 1: The first rib articulates differently from the others, lacks some stabilizing structures present at lower levels [5], and sits in close proximity to the brachial plexus and subclavian vessels. Dysfunction there can produce symptoms referring into the shoulder, arm, or neck, and can contribute to thoracic outlet-type presentations.
Getting a diagnosis
Standard X-ray and MRI are typically “unremarkable “ [4].

Musculoskeletal ultrasound — performed by a trained operator, in both sagittal and transverse planes, comparing adjacent joints — is the recommended first-line imaging tool, and can directly visualize effusion, posterior costotransverse ligament thickening, and vascular changes in chronic cases [1].

Clinically, the most reliable diagnostic approach is hands-on: palpation of the rib head and costotransverse joint, spring testing of rib mobility, and directional movement assessment to determine which joint has shifted and in what direction. This is something I perform as part of every thoracic intake evaluation.
Treatment
Management of costovertebral and costotransverse dysfunction in hypermobility requires layering several approaches — because repositioning the joint addresses the acute problem, but it won't hold without addressing the underlying vulnerability.
Manual therapy and rib alignment(clinical expertise)
Hands-on rib assessment and targeted mobilization is the most direct path to acute pain relief. This involves identifying which rib(s) have shifted, understanding the direction of the dysfunction, and using specific manual techniques to guide the joint back into a functional position. In a hypermobile patient, this is about precision, not force — finding the right contact point and direction, then providing controlled input.
I also teach self-mobilization techniques that patients can use at home for minor shifts. These work well in many presentations and are an important part of building self-efficacy and day-to-day management. In cases of significant ligamentous instability, though, manual correction — whether by a clinician or self-applied — may provide temporary relief while the joint continues to shift with movement. This isn't a failure of technique; it's a signal that the underlying laxity needs to be addressed more directly.
Core and postural rehabilitation(clinical expertise)
Active stabilization is the foundation of long-term management. Work includes diaphragmatic breathing mechanics, thoracic postural control and proprioception, and progressive activation of the deep stabilizing system — transversus abdominis, thoracic multifidus, serratus anterior, and intercostals. The goal is to build an active system capable of compensating for what the passive ligamentous system can't fully provide.
Strength and endurance training(clinical expertise)
Once foundational control is established, building endurance in the thoracic paraspinals, scapular stabilizers, and rotational system reduces fatigue-driven recurrence — one of the most consistent drivers of episodes in this population.
Taping(clinical expertise)
Kinesiology or rigid taping can provide proprioceptive feedback and reduce subluxation frequency during daily activities or exercise. Best used as a temporary adjunct during the rehabilitation process, not as a standalone long-term solution.
Injection therapy(research-supported for inflammation; emerging for instability)
Published research supports ultrasound-guided costotransverse joint injection for thoracic back pain with an inflammatory component [Yoon et al., 2016, cited in 1], and ultrasound guidance is also recommended as essential in anti-inflammatory small joint infiltration [1].
For patients with significant or recurrent ligamentous laxity at the rib-spine junction, prolotherapy — injection of a proliferant (typically dextrose solution) into the affected ligaments and joint capsule — targets the underlying structural laxity rather than the inflammatory response. This is performed by a trained prolotherapist or physiatrist. The evidence base for prolotherapy specifically at the posterior costovertebral and costotransverse junctions in a hypermobile population is currently limited to clinical practice descriptions — no controlled trials exist for this specific application. The rationale is mechanistically sound, and it's something I coordinate around for patients in this population for whom PT alone hasn't produced durable change. If you're interested in exploring it, I'm happy to help identify appropriate providers and coordinate care.
If this sounds like your experience
If you've been living with this kind of pain — told it's muscular without further explanation, gotten normal cardiac workups, or had the maddening experience of feeling something go out and having no one be able to tell you what it is — I want you to know it has a name, a mechanism, and a treatment path.
Costovertebral and costotransverse assessment and treatment in the hypermobility population is an area I've focused on specifically in my practice, and it's something I take seriously. If you're ready to get some real answers, I'd love to be part of your care team.
Have questions or want more information? Click button below to contact me
References
Del Chiaro A, Ciampi B, Franzoni F, Miccoli M, Galletti S, Stella SM. Inflammatory disease of the costotransverse joints: US evaluation in 15 symptomatic patients. J Ultrasound. 2022;25(2):167-175.
Erwin WM, Jackson PC, Homonko DA. Innervation of the human costovertebral joint: implications for clinical back pain syndromes. J Manipulative Physiol Ther. 2000;23(6):395-403.
Groen GJ, Baljet B, Boekelaar AB, Drukker J. Branches of the thoracic sympathetic trunk in the human fetus. Anat Embryol (Berl). 1987;176(4):401-411.
Arroyo JF, Jolliet P, Junod AF. Costovertebral joint dysfunction: another misdiagnosed cause of atypical chest pain. Postgrad Med J. 1992;68(802):655-659.
Madeka I, Alaparthi S, Moreta M, et al. A Review of Slipping Rib Syndrome: Diagnostic and Treatment Updates to a Rare and Challenging Problem. J Clin Med. 2023;12(24):7671.
Gilmer G, Crasta N, Tanaka MJ. The effect of sex hormones on joint ligament properties: a systematic review and meta-analysis. Am J Sports Med. 2025;53(11):2738-2748.
Heitz NA, Eisenman PA, Beck CL, Walker JA. Hormonal changes throughout the menstrual cycle and increased anterior cruciate ligament laxity in females. J Athl Train. 1999;34(2):144-149.